
Persistent Transmission of HCV among Men Who Have Sex with Men despite Widespread Screening and Treatment with Direct-Acting Antivirals
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Population of Acutely Infected HCV Genotype 1a Individuals
2.2. Viral Sequencing of the Non-Structural Proteins 5A and 5B
2.3. Phylogenetic Analysis to Evaluate Transmission Clustering Patterns
3. Results
3.1. Study Population
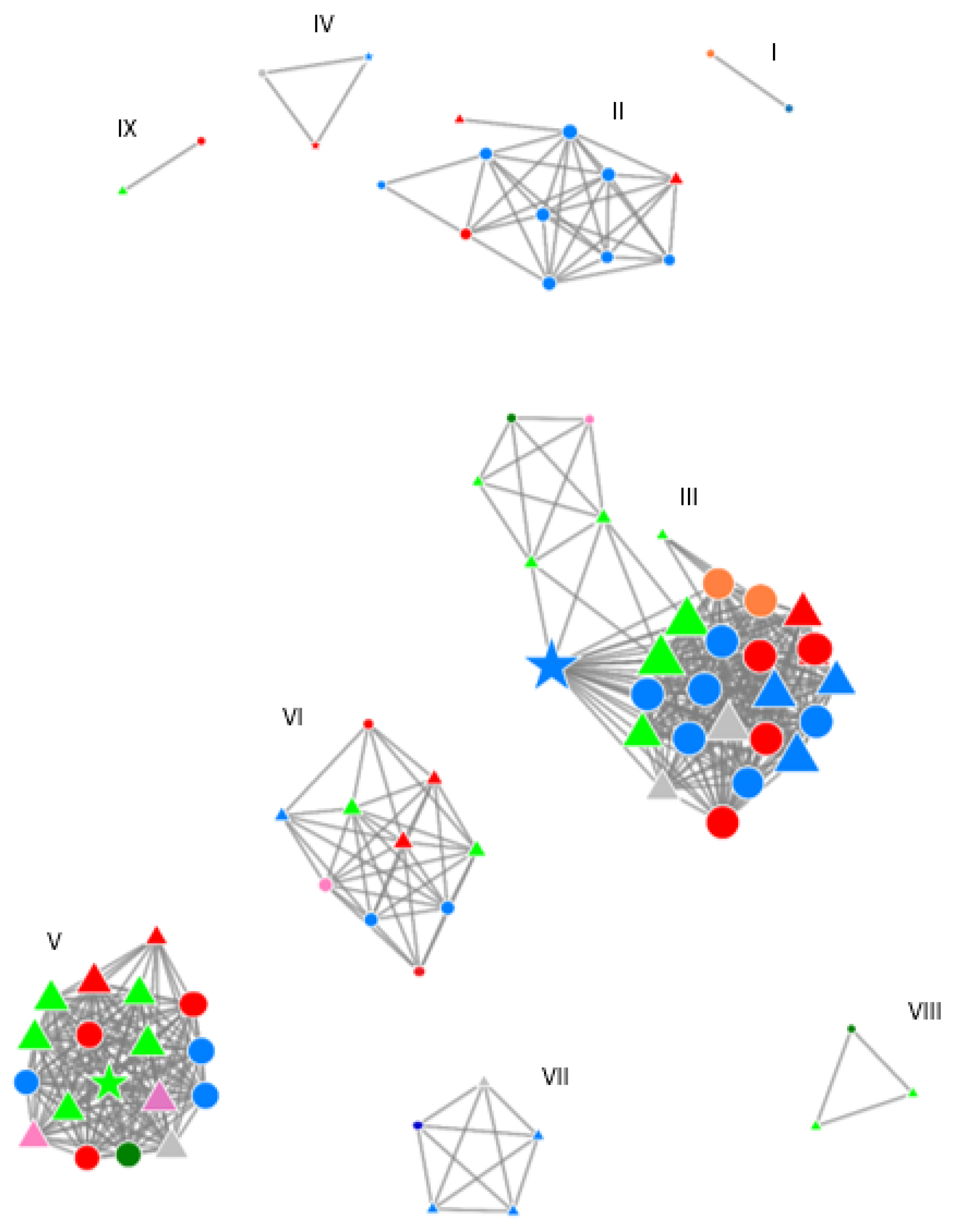
3.2. Recently Acquired HCV Infections in The Netherlands and Belgium Are Highly Clustered
3.3. Clusters Persist after Continuously Monitoring and Broadened Access of DAA Therapy in The Netherlands
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Global Hepatitis Report 2017; Geneva: 2017 CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- The Lancet HIV. Microelimination could be a big deal for HCV and HIV services. Lancet HIV 2018, 5, e605. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Wiktor, S.; Colombo, M.; Thursz, M.; Foundation, E.I.L. Micro-elimination—A path to global elimination of hepatitis C. J. Hepatol. 2017, 67, 665–666. [Google Scholar] [CrossRef] [PubMed]
- Boerekamps, A.; van den Berk, G.E.; Lauw, F.N.; Leyten, E.M.; van Kasteren, M.E.; van Eeden, A.; Posthouwer, D.; Claassen, M.A.; Dofferhoff, A.S.; Verhagen, D.W.M.; et al. Declining Hepatitis C Virus (HCV) Incidence in Dutch Human Immunodeficiency Virus-Positive Men Who Have Sex With Men After Unrestricted Access to HCV Therapy. Clin. Infect. Dis. 2018, 66, 1360–1365. [Google Scholar] [CrossRef] [PubMed]
- Ingiliz, P.; Martin, T.C.; Rodger, A.; Stellbrink, H.J.; Mauss, S.; Boesecke, C.; Mandorfer, M.; Bottero, J.; Baumgarten, A.; Bhagani, S.; et al. HCV reinfection incidence and spontaneous clearance rates in HIV-positive men who have sex with men in Western Europe. J. Hepatol. 2017, 66, 282–287. [Google Scholar] [CrossRef]
- Berenguer, J.; Gil-Martin, A.; Jarrin, I.; Montes, M.L.; Dominguez, L.; Aldamiz-Echevarria, T.; Téllez, M.J.; Santos, I.; Troya, J.; Losa, J.E.; et al. Reinfection by hepatitis C virus following effective all-oral direct-acting antiviral drug therapy in HIV/hepatitis C virus coinfected individuals. AIDS 2019, 33, 685–689. [Google Scholar] [CrossRef]
- Hoornenborg, E.; Achterbergh, R.C.A.; Schim van der Loeff, M.F.; Davidovich, U.; Hogewoning, A.; de Vries, H.J.C.; Schinkel, J.; Prins, M.; Van De Laar, T.J. MSM starting preexposure prophylaxis are at risk of hepatitis C virus infection. AIDS 2017, 31, 1603–1610. [Google Scholar] [CrossRef]
- Vuylsteke, B.; Reyniers, T.; De Baetselier, I.; Nostlinger, C.; Crucitti, T.; Buyze, J.; Kenyon, C.; Wouters, K.; Laga, M. Daily and event-driven pre-exposure prophylaxis for men who have sex with men in Belgium: Results of a prospective cohort measuring adherence, sexual behaviour and STI incidence. J. Int. AIDS Soc. 2019, 22, e25407. [Google Scholar] [CrossRef]
- Ramiere, C.; Charre, C.; Miailhes, P.; Bailly, F.; Radenne, S.; Uhres, A.C.; Brochier, C.; Godinot, M.; Chiarello, P.; Pradat, P.; et al. Patterns of Hepatitis C Virus Transmission in Human Immunodeficiency Virus (HIV)-infected and HIV-negative Men Who Have Sex With Men. Clin. Infect. Dis. 2019, 69, 2127–2135. [Google Scholar] [CrossRef]
- van de Laar, T.; Pybus, O.; Bruisten, S.; Brown, D.; Nelson, M.; Bhagani, S.; Vogel, M.; Baumgarten, A.; Chaix, M.-L.; Fisher, M.; et al. Evidence of a large, international network of HCV transmission in HIV-positive men who have sex with men. Gastroenterology 2009, 136, 1609–1617. [Google Scholar] [CrossRef]
- Hullegie, S.J.; Claassen, M.A.; van den Berk, G.E.; van der Meer, J.T.; Posthouwer, D.; Lauw, F.N.; Leyten, E.M.; Koopmans, P.P.; Richter, C.; van Eeden, A.; et al. Boceprevir, peginterferon and ribavirin for acute hepatitis C in HIV infected patients. J. Hepatol. 2016, 64, 807–812. [Google Scholar] [CrossRef]
- Boerekamps, A.; De Weggheleire, A.; van den Berk, G.E.; Lauw, F.N.; Claassen, M.A.A.; Posthouwer, D.; Bierman, W.F.; Hullegie, S.J.; Popping, S.; Vijver, D.A.C.M.V.D.; et al. Treatment of acute hepatitis C genotypes 1 and 4 with 8 weeks of grazoprevir plus elbasvir (DAHHS2): An open-label, multicentre, single-arm, phase 3b trial. Lancet Gastroenterol. Hepatol. 2019, 4, 269–277. [Google Scholar] [CrossRef]
- Christiansen, M.T.; Hullegie, S.J.; Schutten, M.; Einer-Jensen, K.; Tutill, H.J.; Breuer, J.; Rijnders, B. Use of whole genome sequencing in the Dutch Acute HCV in HIV study: Focus on transmitted antiviral resistance. Clin. Microbiol. Infect. 2017, 23, 123.e1–123.e4. [Google Scholar] [CrossRef] [PubMed]
- Popping, S.; Verwijs, R.; Cuypers, L.; Claassen, M.; van den Berk, G.; De Weggheleire, A.; Arends, J.E.; Boerekamps, A.; Molenkamp, R.; Koopmans, M.P.; et al. Transmission of NS5A resistance associated substitutions among men-who-have-sex-with-men recently infected with hepatitis C virus genotype 1a. Clin. Infect. Dis. 2020, 71, e215–e217. [Google Scholar] [CrossRef] [PubMed]
- Altschul, S.F.; Gish, W.; Miller, W.; Myers, E.W.; Lipman, D.J. Basic local alignment search tool. J. Mol. Biol. 1990, 215, 403–410. [Google Scholar] [CrossRef]
- Trifinopoulos, J.; Nguyen, L.T.; von Haeseler, A.; Minh, B.Q. W-IQ-TREE: A fast online phylogenetic tool for maximum likelihood analysis. Nucleic Acids Res. 2016, 44, W232–W235. [Google Scholar] [CrossRef] [PubMed]
- Kalyaanamoorthy, S.; Minh, B.Q.; Wong, T.K.F.; von Haeseler, A.; Jermiin, L.S. ModelFinder: Fast model selection for accurate phylogenetic estimates. Nat. Methods 2017, 14, 587–589. [Google Scholar] [CrossRef]
- Guindon, S.; Dufayard, J.F.; Lefort, V.; Anisimova, M.; Hordijk, W.; Gascuel, O. New algorithms and methods to estimate maximum-likelihood phylogenies: Assessing the performance of PhyML 3.0. Syst. Biol. 2010, 59, 307–321. [Google Scholar] [CrossRef]
- Hassan, A.S.; Pybus, O.G.; Sanders, E.J.; Albert, J.; Esbjornsson, J. Defining HIV-1 transmission clusters based on sequence data. AIDS 2017, 31, 1211–1222. [Google Scholar] [CrossRef]
- CDC. MicrobeTrace: CDC; 2020. Available online: https://microbetrace.cdc.gov/MicrobeTrace/ (accessed on 27 January 2020).
- van Sighem, A.; Wit, F.; Boyd, A.; Smit, C.; Matser, A.; Reiss, P. Monitoring Report 2019. Human Immunodeficiency Virus (HIV) Infection in The Netherlands. Amsterdam: Stichting HIV Monitoring. 2019. Available online: www.hiv-monitoring.nl (accessed on 26 August 2020).
- Smit, C.; Boyd, A.; Rijnders, B.J.A.; van de Laar, T.J.W.; Leyten, E.M.; Bierman, W.F.; Brinkman, K.; Claassen, M.A.; Hollander, J.D.; Boerekamps, A.; et al. HCV micro-elimination in individuals with HIV in the Netherlands 4 years after universal access to direct-acting antivirals: A retrospective cohort study. Lancet HIV 2021, 8, e96–e105. [Google Scholar] [CrossRef]
- Stephanie Popping, B.N.; Rijnders, B.; van Kampen, J.; Verbon, A.; Boucher, C.; van de Vijver, D. Targeted HCV core antigen monitoring among HIV-positive men who have sex with men is cost-saving. J. Virus Erad. 2019, 5, 179–190. [Google Scholar] [CrossRef]
- Salazar-Vizcaya, L.; Kouyos, R.D.; Fehr, J.; Braun, D.; Estill, J.; Bernasconi, E.; Delaloye, J.; Stöckle, M.; Schmid, P.; Rougemont, M.; et al. On the potential of a short-term intensive intervention to interrupt HCV transmission in HIV-positive men who have sex with men: A mathematical modelling study. J. Viral Hepat. 2018, 25, 10–18. [Google Scholar] [CrossRef]
- Amsterdam Medisch Centrum, SOA AIDS Nederland. NoMoreC Projecct: 2018. Available online: https://nomorec.nl/home (accessed on 4 December 2018).
- Jongen, V.W.; van Rooijen, M.S.; Schim van der Loeff, M.F.; Newsum, A.M.; de Vos Klootwijk, L.; Hoornenborg, E.; Hogewoning, A.; van der Valk, M.; Berk, G.E.V.D.; Prins, M.; et al. Evaluation of the Hepatitis C Testing Strategy for Human Immunodeficiency Virus-Positive Men Who Have Sex With Men at the Sexually Transmitted Infections Outpatient Clinic of Amsterdam, The Netherlands. Sex. Transm. Dis. 2020, 47, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Salazar-Vizcaya, L.; Kouyos, R.D.; Metzner, K.J.; Caraballo Cortes, K.; Boni, J.; Shah, C.; Fehr, J.; Braun, D.L.; Bernasconi, E.; Mbunkah, H.A.; et al. Changing Trends in International Versus Domestic HCV Transmission in HIV-Positive Men Who Have Sex With Men: A Perspective for the Direct-Acting Antiviral Scale-Up Era. J. Infect. Dis. 2019, 220, 91–99. [Google Scholar] [CrossRef]
- Abravanel, F.; Métivier, S.; Chauveau, M.; Péron, J.-M.; Izopet, J. Transmission of HCV NS5A Inhibitor–Resistant Variants Among HIV-Infected Men Who Have Sex With Men. Clin. Infect. Dis. 2016, 63, 1271–1272. [Google Scholar] [CrossRef]
- Koopsen, J.; Parker, E.; Han, A.X.; van de Laar, T.; Russell, C.; Hoornenborg, E.; Prins, M.; van der Valk, M.; Schinkel, J. Hepatitis C Virus Transmission Among Men Who Have Sex With Men in Amsterdam: External Introductions May Complicate Microelimination Efforts. Clin. Infect. Dis. 2021, 72, e1056–e1063. [Google Scholar] [CrossRef] [PubMed]
- Cotte, L.; Cua, E.; Reynes, J.; Raffi, F.; Rey, D.; Delobel, P.; Gagneux-Brunon, A.; Jacomet, C.; Palich, R.; Laroche, H.; et al. Hepatitis C virus incidence in HIV-infected and in preexposure prophylaxis (PrEP)-using men having sex with men. Liver Int. 2018, 38, 1736–1740. [Google Scholar] [CrossRef] [PubMed]
- Charre, C.; Cotte, L.; Kramer, R.; Miailhes, P.; Godinot, M.; Koffi, J.; Scholtès, C.; Ramière, C. Hepatitis C virus spread from HIV-positive to HIV-negative men who have sex with men. PLoS ONE 2018, 13, e0190340. [Google Scholar] [CrossRef]
- Dutch Association of HIV Treating Physicians. HIV Pre-Expositie Profylaxe (PrEP) Richtlijn Nederland. 2019. Available online: http://nvhb.nl/wp-content/uploads/2019/04/PrEP-richtlijn-Nederland-versie-2-dd-15-april-2019.pdf (accessed on 26 August 2022).
- de Vos, A.S.; van der Helm, J.J.; Matser, A.; Prins, M.; Kretzschmar, M.E. Decline in incidence of HIV and hepatitis C virus infection among injecting drug users in Amsterdam; evidence for harm reduction? Addiction 2013, 108, 1070–1081. [Google Scholar] [CrossRef]
- Grady, B.P.; Vanhommerig, J.W.; Schinkel, J.; Weegink, C.J.; Bruisten, S.M.; Lindenburg, C.E.; Prins, M. Low incidence of reinfection with the hepatitis C virus following treatment in active drug users in Amsterdam. Eur. J. Gastroenterol. Hepatol. 2012, 24, 1302–1307. [Google Scholar] [CrossRef]
- Vanhommerig, J.W.; Lambers, F.A.; Schinkel, J.; Geskus, R.B.; Arends, J.E.; van de Laar, T.J.; Lauw, F.N.; Brinkman, K.; Gras, L.; Rijnders, B.J.A.; et al. Risk Factors for Sexual Transmission of Hepatitis C Virus Among Human Immunodeficiency Virus-Infected Men Who Have Sex With Men: A Case-Control Study. Open Forum. Infect. Dis. 2015, 2, ofv115. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Phylogenetic Cluster/Pair | I | II | III | IV | V | VI | VII | VIII | IX |
|---|---|---|---|---|---|---|---|---|---|
| Included 2013–2014 | 2 | 7 | 13 | 1 | 7 | 5 | 1 | 1 | 1 |
| Included 2016–2018 | 0 | 3 | 15 | 2 | 11 | 5 | 4 | 2 | 1 |
| Total number of MSM | 2 | 10 | 28 | 3 | 18 | 10 | 5 | 3 | 2 |
| Mean genetic distance | 0.7 | 1.9 | 1.9 | 1.4 | 2.1 | 2.1 | 1.6 | 0.4 | 1.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popping, S.; Cuypers, L.; Claassen, M.A.A.; van den Berk, G.E.; De Weggheleire, A.; Arends, J.E.; Boerekamps, A.; Molenkamp, R.; Koopmans, M.P.G.; Verbon, A.; et al. Persistent Transmission of HCV among Men Who Have Sex with Men despite Widespread Screening and Treatment with Direct-Acting Antivirals. Viruses 2022, 14, 1953. https://doi.org/10.3390/v14091953
Popping S, Cuypers L, Claassen MAA, van den Berk GE, De Weggheleire A, Arends JE, Boerekamps A, Molenkamp R, Koopmans MPG, Verbon A, et al. Persistent Transmission of HCV among Men Who Have Sex with Men despite Widespread Screening and Treatment with Direct-Acting Antivirals. Viruses. 2022; 14(9):1953. https://doi.org/10.3390/v14091953
Chicago/Turabian StylePopping, Stephanie, Lize Cuypers, Mark A. A. Claassen, Guido E. van den Berk, Anja De Weggheleire, Joop E. Arends, Anne Boerekamps, Richard Molenkamp, Marion P. G. Koopmans, Annelies Verbon, and et al. 2022. "Persistent Transmission of HCV among Men Who Have Sex with Men despite Widespread Screening and Treatment with Direct-Acting Antivirals" Viruses 14, no. 9: 1953. https://doi.org/10.3390/v14091953